There is a great deal written about severe aortic stenosis. Most of it is accurate, and most of it says the same thing. This piece is written to add what the standard references tend to leave out, not because it is obscure, but because it is the kind of understanding that accumulates at the bedside over many years and many valves, rather than in a summary paragraph.
It is written for three readers at once: the patient or family trying to understand a diagnosis; the student who wants the clinical picture stated with precision; and the colleague who already knows the textbook and is interested in the nuance. I have tried not to shortchange any of the three.
The most useful frame I can offer is this. Aortic stenosis is best understood not as a single thing, but as the space between two ways of knowing it: what the patient feels, and what the physician observes. Almost every avoidable delay in this disease lives somewhere in that space.
The Condition, Stated Precisely
The aortic valve is the heart’s final gateway, the structure through which the entire cardiac output passes on its way to the body. Across an average lifetime, it opens and closes in the region of three billion times.
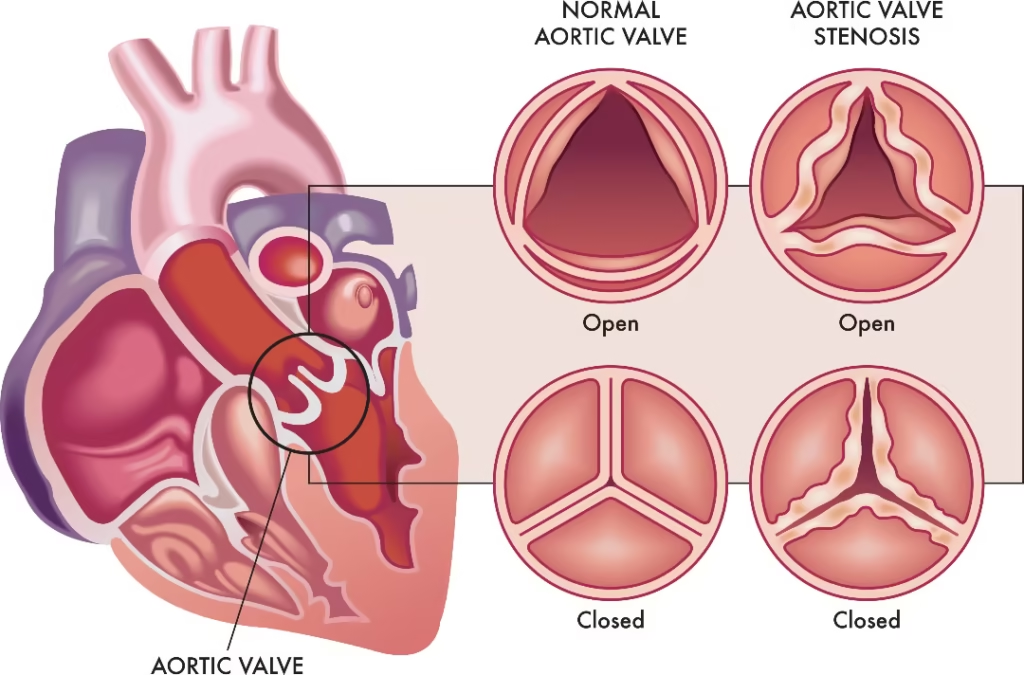
In aortic stenosis, the valve progressively fails to open fully. The left ventricle must generate steadily higher pressure to maintain forward flow, and over time it remodels in response; it hypertrophies, it stiffens, and eventually its function declines.
Severity is defined by international consensus on objective grounds: an aortic valve area below 1.0 cm squared, a mean transvalvular gradient of 40 mmHg or higher, or a peak jet velocity of 4.0 m per second or higher. A normal valve opens to roughly 3-4 cm².
These numbers matter, but as we will see, they can also mislead, and knowing when they mislead is one of the things that separates careful practice from routine reporting.
Etiology Is Not Incidental — It Is Prognostic
The first point that the standard patient-facing summary tends to underplay: the cause of aortic stenosis is not merely a piece of history-taking. It predicts the trajectory of the disease and frames the eventual intervention.
There are three principal origins. The first is calcific aortic valve disease, the most common in older adults. It is tempting, and it is the version most people find online, to describe this as simple wear and tear, the valve “hardening with age.” That description is biologically incorrect.
Calcific aortic stenosis is an active, regulated process: lipid infiltration, chronic inflammation, and frank osteogenic differentiation within the leaflet, with the same cellular machinery the body uses to build bone. The valve does not passively rust. It is, in a real sense, ossifying.
This matters because it explains the second point, why no medication has yet been able to stop it, and because it places aortic stenosis in the same biological family as atherosclerosis rather than treating it as mechanical attrition.
The second origin is the bicuspid aortic valve, a valve formed with two cusps rather than three, present in roughly one to two per cent of the population.
It is not simply a valve that wears out earlier. It frequently accompanies an aortopathy, an abnormality of the aortic wall itself, that can outlive clinical attention to the valve.
The lesson, particularly for students and referring physicians, is that a bicuspid valve is a reason to look at the aorta, not just the leaflets.
The third is rheumatic heart disease valve scarring following inadequately treated streptococcal infection in childhood. It has receded from high-income countries but remains a substantial reality across much of the world, including parts of South Asia.
Its physiology, commissural fusion rather than nodular calcification, behaves differently, and a clinician who only ever sees calcific disease can be caught out by it.
“The mechanism does not just explain the disease. It should set the surveillance interval, not only the eventual operation.”
Symptoms: What The Patient Feels and What Almost No One Reports
The recognised symptoms of severe aortic stenosis are exertional breathlessness, chest tightness with activity, light-headedness or frank syncope on exertion, unusual fatigue, and, at times, an awareness of a rapid or fluttering heartbeat.
These are accurate and are everywhere online.
Here is what is not everywhere online, and it is the single most important thing I can tell a patient or a referring colleague. Many patients with severe aortic stenosis will tell you, sincerely, that they have no symptoms.
They are frequently mistaken, not because they are concealing anything, but because the human response to a slowly narrowing valve is not to report breathlessness. It is to quietly stop doing the things that provoke it.
The walk becomes shorter. The stairs are taken less often, or more slowly, or avoided. The evening routine is allowed to lapse. None of this is experienced as illness. It is experienced as a reasonable adjustment, or simply as age.
In clinical terms, a meaningful proportion of “asymptomatic” severe aortic stenosis is, on objective testing, symptom-concealed severe aortic stenosis.
This is why a reassuring clinic conversation is one of the least reliable instruments we have, and why objective functional assessment, a structured treadmill evaluation, the trajectory of natriuretic peptides, and serial changes in left ventricular longitudinal strain interrogate what the history cannot.
For the patient reading this, the practical translation is gentle but specific. If an older person you love has not complained of anything but has visibly become more careful, that observation is itself clinical information worth bringing to a cardiologist.
Signs: What the Physician Observes
Signs are another way of knowing the disease that the trained examiner detects, regardless of what the patient reports. They are the reason an unhurried clinical examination retains its quiet power even in an era of advanced imaging.
A characteristic ejection systolic murmur that the patient will never hear themselves. A carotid upstroke that rises more slowly and with lower amplitude than it should, the parvus et tardus pulse, which, to an attentive hand, signals a haemodynamically significant valve before any scan is ordered.
A narrowing pulse pressure. And then the arbiter: the echocardiogram, which quantifies, with precision, what the body itself cannot articulate: valve area, gradient, jet velocity, ventricular response.
The elegant truth is worth stating plainly, because it reframes the patient’s role rather than frightening them: a sign noted years before symptoms, a murmur recorded once, on an old file, and never traced, is one of the most common missed beginnings of this disease.
The valve did not hide. The thread was simply not followed. Proactive care is, in large part, the discipline of following that thread.
The Diagnosis That Misleads: Low-Flow, Low-Gradient Aortic Stenosis
If there is one section of this article that justifies its existence in an already crowded field, it is this one.
The instinct shared by patients, students early in training, and even some experienced clinicians is that higher numbers mean greater danger, that a high gradient is alarming and a lower gradient is reassuring.
In severe aortic stenosis, that instinct can be precisely inverted.
The transvalvular gradient is flow-dependent. It reflects not only how narrow the valve is, but how forcefully the ventricle is pushing through it.
When the ventricle is strong, a critically narrowed valve produces a high gradient. But when the ventricle begins to fail, the number falls. Not because the valve has improved. Because the heart is losing.
“A report that suddenly looks quieter deserves more attention, not less.”
This entity, classical low-flow, low-gradient severe aortic stenosis with reduced ejection fraction, and its paradoxical counterpart with preserved ejection fraction, is the patient most likely to be falsely reassured.
A discordant valve area and gradient is not a reason for comfort; it is an indication for further interrogation: dobutamine stress echocardiography to assess flow reserve and distinguish true severe from pseudosevere disease, or aortic valve calcium scoring on CT for a flow-independent estimate of severity.
The valve, today, is eminently replaceable. The misclassification is the lesion that hurts the patient.
Why No Tablet Closes This Door
Patients ask, reasonably, for the medicine that will reverse this. Students ask why, given how precisely we understand biology, there is still no pharmacological therapy.
The honest answer is one of the more humbling statements in cardiology, and it deserves to be made plainly rather than glossed.
We understand the mechanism of calcific aortic stenosis in considerable molecular detail. We know it shares pathways with atherosclerosis.
It was therefore entirely rational to expect that lipid-lowering therapy might slow it, and this was tested properly, in well-designed randomised controlled trials. It did not work.
The valve, once the osteogenic process is established, does not respond to the medicines that so effectively modify vascular disease.
There is currently no medical therapy that alters the natural history of severe aortic stenosis. Symptoms and consequent heart failure can be managed; the disease itself is, at present, mechanical in its solution.
The Shape of Modern Treatment
For decades, the only definitive treatment was surgical aortic valve replacement, and for a fit patient, it remains an excellent and durable operation.
The transformation of the field, and I say this having performed India’s first transcatheter aortic valve implantation in 2010, is that valve replacement is no longer gated by whether a patient can withstand open-heart surgery.
Transcatheter aortic valve implantation delivers a new valve through a catheter, typically from the femoral artery, with the heart beating and without sternotomy.
Across a sequence of landmark randomised trials, the evidence base has matured from high surgical risk through intermediate risk to selected low-risk patients.
The consequence is a genuine shift in where the difficulty now lies. Feasibility is largely solved. The discipline of the present era is selection, which patient, which valve, by which route, and above all, when.
The decision belongs to a Heart Team in which an interventional cardiologist, a cardiac surgeon and an imaging specialist reason together.
For most patients with severe symptomatic aortic stenosis today, the meaningful question is no longer whether they can be treated. It is whether they will be assessed in time for the answer to matter.
There is also a moving frontier worth stating with care, because it is easy to overstate.
In carefully selected patients with severe aortic stenosis who have not yet declared symptoms, contemporary evidence suggests earlier intervention may reduce subsequent hospitalisation compared with watchful waiting.
This should be read precisely: the clearest signal is fewer hospitalisations rather than a dramatic difference in survival, and patient selection becomes more important, not less.
But the long-held instinct to wait until the ventricle declares the disease for us is, rightly, being re-examined.
A Global Lens
One reason general statements about aortic stenosis travel poorly across borders is that the patient is not the same everywhere.
In high-income registries, this is largely a disease of the eighties. In much of South Asia, a substantial proportion of patients reaching valve intervention are considerably younger.
This pattern is driven partly by a high prevalence of bicuspid disease and by the continued presence of rheumatic heart disease.
The implication, for colleagues anywhere, is a caution against importing age thresholds and selection habits wholesale.
Biology is universal; the population is not. This is also why building and trusting regional evidence is not parochial; it is methodologically necessary.
What I Would Ask Every Reader to Take From This
To the patient or the family, the most reassuring step in heart health is rarely dramatic. It is a considered conversation and a stethoscope placed in time.
If there is a murmur once mentioned and never explored, or an older person who has quietly become more careful, those are not trivia. They are invitations to a proactive assessment, and proactive assessment is where this disease is won.
To the student: hold on to the distinction between what is felt and what is observed, and to the single most counter-intuitive fact in this disease that the gradient can fall as the danger rises.
To the colleague: I would value knowing how you are now weighing strain imaging and calcium scoring in your discordant cases, and where the threshold for intervening in the asymptomatic patient is settling in your own practice.
This remains, productively, an open conversation.
“The valve has become replaceable. The missed conversation has not.”

