It Began With One Question.
In 2010, an eighty-year-old gentleman from Dehradun travelled down through the hills with his son to my consultation room at Medanta. He had been breathless for months. The simple climb from his veranda to his garden had become a daily test of will. His family had brought him this distance, well over two hundred kilometres from the foothills of Uttarakhand to Gurugram, after two leading hospitals had told them, kindly but unambiguously, that nothing more could be done.
His diagnosis was severe calcific aortic stenosis. His aortic valve, the gateway through which all oxygen-rich blood leaves the heart for the body, had hardened and narrowed to a slit. His heart was working three to four times harder than mine to push blood through it. Open-heart surgery in his case carried a mortality risk in excess of thirty per cent. He had been advised to go home and rest.
He looked at me across the desk, his son sitting quietly beside him. He had carried his medical files in a worn leather folder. And he asked one question.
“Doctor, is there anything else?”
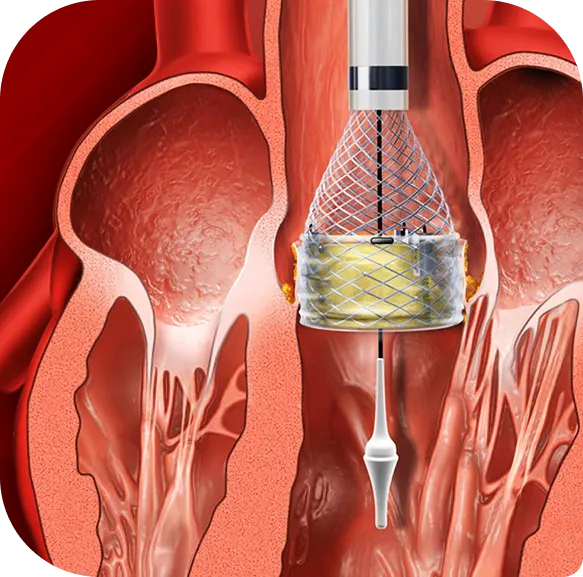
There was. But it had never been done in India without opening the chest. I told him about a procedure I had been studying, a way to replace his aortic valve through a thin catheter passed from the groin, while his heart kept beating, while he stayed awake. I told him about the risks. I told him about the uncertainties. He listened with the calm patience of a man who has lived through many decades and learned to weigh things carefully. Then he said, simply:
“When?”
Three days after that procedure, he walked out of Medanta on his own feet. He told me he had not walked that easily in five years.
That was India’s first percutaneous aortic valve implantation without open-heart surgery. We now call it TAVI (Transcatheter Aortic Valve Implantation), sometimes also written as TAVR. His question, “Is there anything else?” has shaped every clinical decision I have made for the past sixteen years.
Why 1,000 TAVI Procedures Matter.
This month, our structural heart team at Medanta crossed a milestone that I want to mark publicly, not for the number itself, but for what it represents. We have now performed over 1,000 TAVI procedures.
This is one of the highest individual TAVI volumes in India. But more importantly, it represents one thousand patients, most of them in their seventies and eighties, many of them previously told by other centres that they were beyond help, who today walk, climb stairs, play with their grandchildren, and sleep through the night without breathlessness.
Each of those thousand patients is a question answered. A family reunited. A life that very nearly ended in a different conversation.
Severe Aortic Stenosis in India: The Question We Have Not Yet Asked.
Even as I mark this milestone, I find myself returning to a number that appears on no congratulatory note.
Three hundred thousand. That is the estimated number of Indian patients currently living with severe aortic stenosis who would be candidates for valve replacement. The prevalence of aortic stenosis in patients undergoing echocardiography in India is approximately 7.3 per cent, broadly comparable to global figures, with degenerative calcific disease being the dominant cause in elderly patients.
Of these three hundred thousand, only a fraction will reach a centre that offers TAVI in India. Most will be told, as my first patient was told, before his family brought him down from Dehradun, that surgery is too risky. Many will be sent home with medication and a recommendation to manage symptoms. In too many cases, the conversation will end there.
This is the gap I want every cardiologist, every general physician, and every Indian family to understand. The science exists. The technology has matured. TAVI is now considered the standard of care globally for elderly patients with symptomatic severe aortic stenosis at high or intermediate surgical risk, and increasingly for selected low-risk patients as well. The PARTNER trials and the Evolut Low Risk trial, published over the past decade, have given the procedure an evidence base that is among the strongest in modern cardiology.
What is missing in India is not capability. It is awareness.
“Inoperable” is sometimes just “no one has looked at the right options.”
What 1,000 TAVI Procedures Have Taught Us About Indian Hearts.
Sixteen years of TAVI work in India, much of it pioneering, much of it building on global advances we have helped adapt for Indian patients, has taught my team several things worth sharing with both peers and patient families.
First, the Indian TAVI patient is younger than the Western average. Studies have shown that approximately sixty per cent of TAVI patients in India are under the age of sixty, a striking contrast to Western registries where the procedure is most often performed in patients above eighty. This is partly explained by the high prevalence of bicuspid aortic valve disease in our population. Close to one in three Indian TAVI candidates have bicuspid anatomy, a rate that is multiples higher than in Caucasian populations. The remainder is explained by differences in life expectancy, presentation patterns, and the way patients reach cardiac care in India. The clinical implication is direct: our outcomes data, our valve selection, and our procedural planning cannot simply be borrowed from Western experience. Indian cardiology must build its own evidence base.
Second, outcomes at high-volume Indian centres are now genuinely comparable to outcomes at leading centres in the United States, the United Kingdom, and Europe. This is not a claim I make lightly. It is supported by data from multiple Indian academic centres, presented at major international meetings of the American College of Cardiology and the European Society of Cardiology, and increasingly published in peer-reviewed journals.
Third, and this is what no statistic can fully capture, recovery transforms not just the patient but the entire family. I have watched grandparents return to family weddings they had quietly assumed they would not live to see. I have watched fathers walk their daughters down the aisle. I have watched widows discover, in their eighties, that they had years of life still ahead of them. These are not small things. They are the entire reason we do this work.
The First TAVI Patient: The Gentleman From Dehradun.
My first TAVI patient, the gentleman who travelled down from Dehradun in 2010 and asked whether there was anything else, went on to live many more years than anyone had predicted. He returned to his hills. He returned to his garden. He returned to the routines of an Indian elder who had been given his life back. At every follow-up echocardiogram in the years that followed, the valve we placed in his heart that November continued to function as it should.
His family wrote to me sometime later. They said:
“You did not just give him years. You gave him the years that mattered most.”
I keep that letter on my desk.
The Future of Structural Heart Care in India.
As I look at the next decade of structural heart care in India, three priorities become clear.
We must train more interventional cardiologists in the TAVI technique, not just at metropolitan centres, but at tier-two cities where access to structural heart specialists remains poor. The expertise required for TAVI, MitraClip, and other transcatheter valve procedures cannot be concentrated only in Delhi, Mumbai, Chennai, and Bengaluru. A patient in Dehradun, in Indore, in Patna, in Vijayawada, deserves the same standard of cardiac care as a patient in Gurugram.
We must work with policymakers, insurers, and device manufacturers to bring procedure costs within reach of more Indian families. TAVI remains a costly procedure, and even with the recent emergence of indigenous Indian valves at lower price points, financial access is still the most significant barrier for the majority of eligible patients. This is not a problem any single hospital or cardiologist can solve. It requires sustained national attention.
And we must collectively, as a profession, stop telling elderly patients that their hearts are beyond help, when often, they are not. Every cardiologist who has practised in India for more than a decade has seen patients who were dismissed by one centre and who went on to live transformed lives after a second opinion at a centre with TAVI experience. These are not exceptional cases. They are increasingly common cases. And they should be expected, not surprising.
The patient who walks into a clinic next week, breathless and tired, deserves the same question my eighty-year-old gentleman from Dehradun asked of me in 2010.
“Is there anything else?”
Almost always, today, there is.

