By Dr Praveen Chandra | Padma Shri | Chairman, Interventional Cardiology, Medanta — The Medicity | Performed India’s first TAVI, 2010
For years I have watched the heart do something quietly heroic. When the aortic valve narrows and hardens with calcium, a condition we call aortic stenosis, the heart does not complain. The left ventricle simply thickens its walls and pushes harder against the obstruction, season after season, until the muscle itself begins to tire. So my patients sit across from me and say they feel fine, even as the breathlessness on the stairs and the fatigue they have blamed on age have already become the valve’s first quiet letters home. The word fine, in my clinic, is the one I have learned to gently question.
Aortic stenosis is among the most common valve conditions of later life, and it is too often dismissed as simply growing old. I have written before, on these same pages, about how it hides. Consider this the next chapter, the one where we do something about it.
The Procedure, and What It Treats
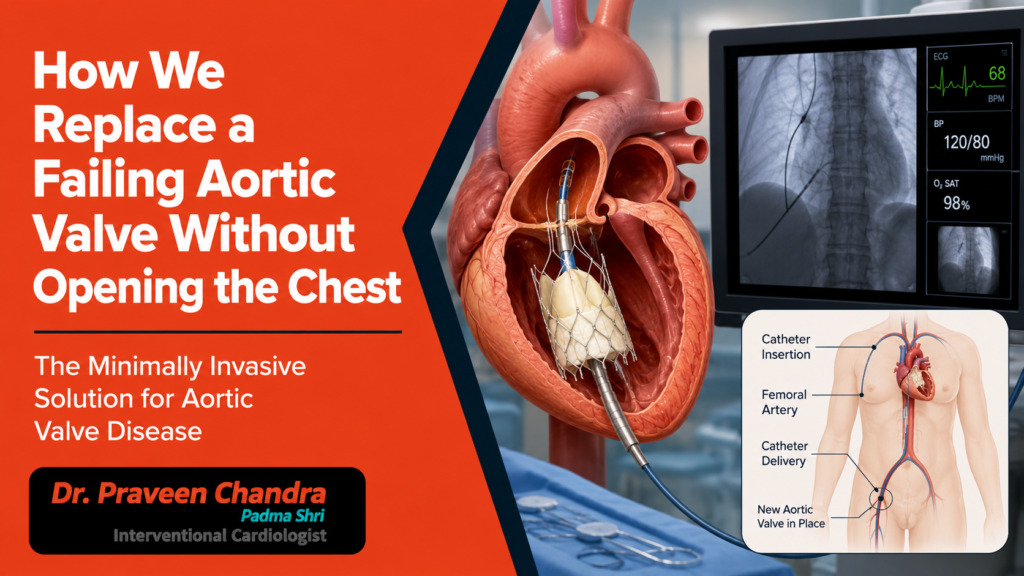
The treatment is TAVI, transcatheter aortic valve implantation, also written as TAVR. Its main purpose is to relieve severe aortic stenosis, the hardened, narrowed valve that strangles the flow of blood leaving the heart. It also allows us to place a fresh valve inside an old surgical valve that has worn out, a procedure we call valve-in-valve, which spares many patients a second open operation. One fact deserves to be widely known, because it changes how seriously people take this condition. No tablet can reopen a calcified valve. Medication can ease the symptoms for a while, but once the valve is severely narrowed and causing trouble, it must be replaced. TAVI does not cure the body’s tendency to lay down calcium; what it does is restore the normal flow the heart has been straining for.
We do not divide the breastbone or stop the heart, and the heart and lung machine that conventional surgery relies on stays switched off. The real work begins before any catheter, on a detailed CT scan of the aortic root. The annulus, the ring the valve sits upon, is seldom a clean circle. It is usually an oval, so we measure both its area and its perimeter, because a single millimetre can change the device we choose. On the day itself, we reach the heart through the femoral artery at the top of the leg, with a sheath only a few millimetres wide. The new valve, made of treated tissue on a fine metal frame, is crimped to the width of a pen and guided up to the heart under live imaging. We watch the depth of the implant with great care, because the heart’s electrical wiring runs just beneath the valve. The instant the valve opens, its leaflets take over, and blood that had been straining through a narrowed slit moves freely again. Most patients are awake or lightly sedated, and the whole procedure is measured in a couple of hours.
Who It Is For, and Who I Hold Back
For a long time TAVI was reserved for patients judged too frail for surgery. That door has opened, and today it is offered across a wide range of surgical risk. The decision is never mine to make alone; it belongs to the heart team, a group of interventional cardiologists, surgeons, imaging specialists and anaesthetists who weigh each patient together.
There is one group where I deliberately step back, and I want to explain why in plain terms, because the reasoning matters. The valve we implant during TAVI is a tissue valve, made from treated biological material, and it does not last forever. Surgical tissue valves have typically needed attention after years, and the very long-term durability of the transcatheter valve, beyond ten years, is still being studied. For an older patient, that lifespan comfortably covers the years ahead. For a younger patient, with two or three decades of life still to come, it may not, and they could face repeat procedures down the line. This is also why the large trials that established TAVI were conducted mainly in older patients, and why international guidelines still favour surgery for most people below the age of around sixty-five. In a younger patient, I would rather place a durable valve surgically now and keep TAVI in reserve as a future option, including the valve-in-valve approach, than spend that one good innings of durability too early. Choosing the right patient is as much a part of this craft as performing the procedure, and knowing when to step back is the quieter half of the skill.
What TAVI Changed, in the World and in India
This field moves quickly, and the past two years have moved it further than most. The EARLY TAVR trial, published in 2024, showed that treating severe aortic stenosis early, even before symptoms arrive, prevented strokes and hospitalisations that watchful waiting did not. On the strength of that evidence, regulators approved TAVI for selected patients with no symptoms at all. International guidance in 2025 went on to name TAVI a first choice for most patients above the age of seventy.
For India, this is a story I have watched from the inside and, in part, helped to begin. When the first of these procedures was performed in this country, it was rare and unfamiliar, available to very few. Today it is an established treatment offered in leading centres, and awareness among families is finally catching up with what is possible. We have moved from a procedure spoken about only at conferences abroad to one we now perform, refine and teach at home. That is a change worth naming plainly.
Precision PCI: Bringing the Same Precision to the Arteries
A narrowed valve is rarely the whole story. Close to half the patients I treat for severe aortic stenosis also carry narrowing in the coronary arteries that feed the heart muscle, and the way we treat those arteries has undergone its own quiet revolution. This is what I mean by Precision PCI.
A standard angiogram shows an artery as a shadow, a silhouette cast by dye. It is a useful map, but a shadow cannot tell you the true width of the vessel, the real burden of plaque hidden in its wall, or whether a stent has fully opened once placed. Precision PCI replaces that guesswork with measurement. Using intravascular imaging, an ultrasound or light-based probe slimmer than the artery itself, we look at the vessel wall from the inside and size the stent exactly. Using physiology, a fine pressure wire passed across a narrowing, we measure whether that narrowing is genuinely starving the muscle, so we treat the blockages that matter and leave the innocent ones alone.
The evidence behind this is now substantial. In patients with complex disease, imaging-guided stenting has been shown to lower the combined risk of cardiac death, heart attack, and a return trip to reopen the same vessel. A stent that is correctly sized and fully expanded fails less often and clots less often, which is the difference between a procedure done and a problem solved. There is something here worth knowing as a patient, too. Not every angioplasty in this country is guided this way; a great many are still performed using the angiogram alone. It is entirely reasonable to ask your cardiologist whether imaging and pressure measurement will be used to guide your stent. To my mind, Precision PCI is the natural next step in interventional cardiology, the same shift from eyeballing to measuring that imaging brought to the valve, and for the right patient it deserves to be the standard rather than the exception.
Life After the Procedure
This is the part patients ask about most. After TAVI, many are sitting up the same evening and home within two or three days. The breathlessness that had crept into every staircase often lifts inside the first week, because the obstruction the heart had been fighting is simply gone. People walk further and sleep flatter, and they return to the work and the grandchildren they had quietly been surrendering. What does long-term care look like? It’s simpler than you think. It just takes a brief course of blood-thinning medication, consistent management of your blood pressure and cholesterol, and a yearly echocardiogram to check on the valve. Just a few smart, everyday habits to ensure lasting peace of mind. For most, life widens again.
Why I Call This Safe, and Mean It
Safe is a word I use carefully, because I owe my patients precision rather than reassurance. In the major trials of lower-risk patients, the risk of death in the first thirty days after TAVI has been well under one in a hundred, with rates of stroke and serious bleeding comparable to or lower than surgery, and a far gentler recovery. At five years, survival has tracked closely with surgery. Precision PCI is inherently safer because it relies on exact measurement. It ensures a stent is perfectly sized, fully expanded, and placed precisely where it will deliver the most impact. A procedure is only ever as safe as the judgement behind it, and that judgement is built one careful case at a time.
Why This Work Belongs at Medanta
What do we do differently at Medanta? We don’t stop at the valve. The very same precision that guides a transcatheter valve into its exact position is the standard we apply to the coronary arteries via Precision PCI. To us, the heart isn’t a collection of separate problems; it’s a single organ. Every treatment we do is designed to make the whole system work in perfect harmony. I performed India’s first transcatheter aortic valve implantation, and I have spent the years since helping to build structural heart intervention in this country and teaching it to colleagues at international meetings. That history is the reason a difficult decision can be made here calmly, and a demanding procedure can feel almost unremarkable for the person living through it. All of it sits within a structural heart programme built over two decades, supported by a complete heart team and advanced imaging, where the valve and the arteries are treated by people who do this work every day.
If the stairs have felt longer lately, or a doctor has mentioned a murmur, please do not wait for the valve to announce itself plainly. Ask for an echocardiogram. It takes about twenty minutes, and it could give you back years.

