By Dr Praveen Chandra | Padma Shri | Chairman, Interventional Cardiology, Medanta — The Medicity | Performed India’s first TAVI, 2010
A particular consultation in the valve clinic has become more frequent in recent years, and it almost always ends with a degree of confusion that the patient is entitled to. The echocardiogram demonstrates a valve that is severely narrowed by every guideline measure. The patient reports feeling well. The recommendation that follows is not surgical, not yet, but careful surveillance. Two messages, severe and wait, sit uncomfortably together in the same conversation. The family leaves the consultation less certain than when they arrived.
This is Stage C aortic stenosis. It is, in my view, the most consequential conversation in valve medicine today, and the most actively contested in the global cardiology literature. The pages that follow are an account of what is, in fact, being weighed in that conversation, written in equal measure for the patient navigating the diagnosis, the trainee approaching the topic for the first time, and the colleague following the evidence as it has shifted beneath us over the past five years.
Defining Stage C precisely
The accepted framework for valvular heart disease, set out by international guidelines including those of the American College of Cardiology and the European Society of Cardiology, recognises four stages. Stage A is where the patient is at risk, the valve is normal, but conditions for disease are present. Stage B is mild to moderate disease without symptoms. Stage C is severe disease without symptoms. Stage D is severe disease with symptoms.
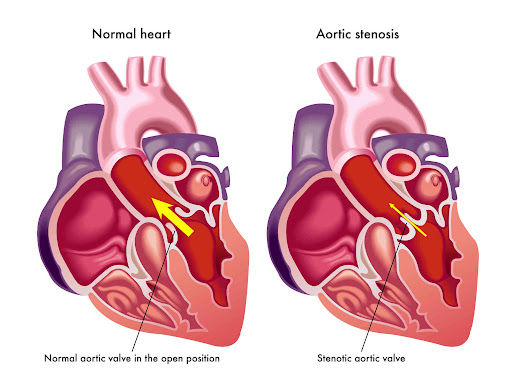
On the echocardiogram, severe aortic stenosis is defined by three concordant findings. The aortic valve opening, normally three to four square centimetres, has narrowed to less than one square centimetre. The mean pressure gradient generated by the left ventricle across the valve is forty millimetres of mercury or higher. The peak velocity of the blood jet through the narrowed opening is four metres per second or above. A patient meeting all three criteria has severe disease by any contemporary international standard.
What makes Stage C clinically demanding is the qualifier that follows the diagnosis. The word asymptomatic should, in theory, be a binary determination. In practice, it is among the more nuanced judgements in clinical cardiology, and the reason for that nuance deserves attention before we proceed.
The qualification is rarely made about ‘asymptomatic’
A meaningful proportion of patients categorised as asymptomatic on careful evaluation are not, in fact, free of symptoms. They have unconsciously adapted to a narrowing valve by reducing what they ask of themselves. The morning walk is taken at a slower pace, or shortened, or quietly discontinued. The stairs are managed one flight at a time. Routines that involve exertion are gradually negotiated away. None of this registers in the patient’s own narrative as illness; it registers as sensible, or as ageing.
The clinical implication is direct. A patient’s self-report that they feel well is not, by itself, sufficient evidence of an asymptomatic state. The careful Stage C evaluation includes the structured questioning of accompanying family members, who are very often the most reliable historians in the room; an objective measure of exercise capacity, typically through a structured treadmill test; and, where indicated, serial measurements of natriuretic peptides and longitudinal strain on echocardiography. A patient may report an absence of symptoms, but an exertional drop in systolic blood pressure indicates otherwise. Clinically, this reclassifies the patient as symptomatic, which fundamentally alters our recommendation for intervention.
“The most useful question in Stage C is rarely, How do you feel?. It’s what have you stopped doing?”
The recurring pattern in the clinic
Rather than relate a specific patient case, I will describe a pattern observable across many consultations, because the pattern teaches more reliably than any single example. A patient is referred with severe aortic stenosis on a recent echocardiogram. They have not been told that their valve is severely narrowed; they have been told to seek an opinion. They sit in the consulting room and, asked how they feel, say they feel well.
It is the family member accompanying them, a spouse, an adult child, occasionally a sibling, who, almost in passing, mentions a particular detail. The morning walk that no longer happens. The temple visit that has become weekly rather than daily. The climb to the upper floor of the house that has been quietly negotiated away. The patient, on hearing this, often agrees mildly that it is so, while remaining convinced that the change is unrelated to anything medical. The structured treadmill assessment that follows then frequently demonstrates what the conversation alone did not: a reduced exercise capacity, a flat blood pressure response, an abnormal rise in pulmonary pressures, or a symptom that emerges with exertion that the patient had not been provoking in daily life.
That sequence, what is said, what is observed, and what is tested, is the architecture of a careful Stage C consultation. It is also why a fifteen-minute clinic encounter, however well-conducted, cannot reliably arbitrate this question. The judgment requires time, family presence, and objective testing of exertional capacity. Where these are not available, the right step is to seek a structural heart team review at a centre with experience of the volume.
Where the global evidence has moved
The international thinking on intervention in Stage C aortic stenosis has shifted measurably over the past five years, and this section is the one I would most encourage trainees and colleagues to read with care. For the patient or family member, the same content is the basis on which a cardiologist today recommends earlier action in some Stage C patients than would have been advised a decade ago.
Three trials in particular define the contemporary evidence base, and they are worth understanding in their proper proportion.
The RECOVERY trial, published in the New England Journal of Medicine in 2020 by a Korean investigator group, examined patients with very severe asymptomatic disease, a peak jet velocity of four point five metres per second or higher, and compared early surgical aortic valve replacement with conservative management. At six-year follow-up, the composite of operative mortality and cardiovascular death occurred in approximately one per cent of patients in the early-surgery arm and in approximately fifteen per cent of those managed conservatively. The threshold was strict and the patient population carefully selected, but the difference was substantial.
The AVATAR trial, published in Circulation in 2022, extended the question to a broader asymptomatic severe population. At thirty-two-month follow-up, the primary composite of all-cause death, acute myocardial infarction, stroke, and unplanned hospitalisation for heart failure occurred in approximately fifteen per cent of patients assigned to early surgery, compared with approximately thirty-five per cent of those managed conservatively. The benefit was driven principally by a reduction in heart failure hospitalisation; the mortality difference, while present, was less marked.
EARLY TAVR, presented at the Transcatheter Cardiovascular Therapeutics meeting in October 2024 and published in the New England Journal of Medicine in early 2025, asked the contemporary version of the question. In nine hundred and one patients across seventy-five centres in the United States and Canada, transcatheter aortic valve replacement was compared with guideline-directed clinical surveillance in asymptomatic severe aortic stenosis confirmed by negative treadmill testing. At a median follow-up of three point eight years, the primary composite of death, stroke, and unplanned cardiovascular hospitalisation occurred in 26.8 per cent of patients in the early-TAVR arm and 45.3 per cent in the surveillance arm, a relative reduction of fifty per cent.
The single most important caveat in interpreting EARLY TAVR is the breakdown of that composite. The reduction was driven principally by unplanned cardiovascular hospitalisation. Mortality alone was 8.4 per cent in the early-TAVR arm and 9.2 per cent in the surveillance arm, a difference that did not reach statistical significance. Stroke occurred in 4.2 per cent and 6.7 per cent, respectively. Furthermore, eighty-seven % of patients initially assigned to surveillance eventually underwent valve replacement during follow-up, with a median time to crossover of approximately eleven months.
The honest summary is therefore as follows. EARLY TAVR establishes that early intervention reduces the likelihood of an unplanned cardiac admission in the years ahead and improves measures of quality of life and ventricular health. It does not, on its primary analysis, demonstrate a mortality benefit at the median follow-up duration tested. The implications for patient selection are more significant after EARLY TAVR, not less; the trial does not constitute a licence to proceed in every Stage C patient, but it does substantially weaken the historical case for indefinite watchful waiting in the carefully evaluated patient.
A further trial worth knowing of is EVOLVED, presented at the same meeting in 2024, which addressed asymptomatic severe aortic stenosis specifically in patients with mid-wall myocardial fibrosis detected on cardiac magnetic resonance imaging. Its overall primary composite endpoint did not reach statistical significance, but secondary endpoints relating to symptom progression and aortic stenosis-related hospitalisation favoured early intervention. The trial is a useful reminder that imaging biomarkers of ventricular response are increasingly relevant to the Stage C decision.
In May 2026, the American College of Cardiology, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons issued a joint statement on aortic valve replacement decision-making, recognising the maturation of the evidence base and the importance of formal Heart Team review in selected Stage C patients. The direction of the international standard is unambiguous, if not yet uniform: the threshold for intervention in Stage C is migrating earlier than it was a decade ago, conditional on careful evaluation and shared decision-making.
How the decision is reached in practice
There is no single test or threshold that determines the recommendation for any individual patient. There is a framework, a Heart Team discussion, and the patient’s own informed preference, which carries particular weight in this decision because the patient is asked to weigh a known intervention against an uncertain natural history. The following are the principal inputs to that discussion, in approximately the order they are considered.
- First, the objective measures of the valve and the ventricle. The severity of stenosis on the most recent echocardiogram, the rate of progression across serial studies, and the response of the left ventricle. Early reductions in longitudinal strain on speckle-tracking imaging may precede a fall in ejection fraction by months or years and are increasingly used as a signal that compensation is failing.
- Second, the structured assessment of exertional capacity. A formal treadmill test, with attention to symptoms provoked by exertion, an abnormal blood-pressure response, a rise in pulmonary pressures, or simply a reduced exercise tolerance for the patient’s age and conditioning. An abnormal exercise test in an apparently asymptomatic patient is one of the most consequential single findings in Stage C evaluation.
- Third, biomarker trajectory. Natriuretic peptides, BNP and NT-proBNP, begin to rise before the ventricle fails clinically. A trajectory rising across serial measurements, even within the laboratory-reported normal range, is a signal that warrants attention in the context of severe valvular disease.
- Fourth, the valve calcium burden quantified by computed tomography. Particularly in women, where conventional gradient thresholds may understate severity, CT-derived calcium scoring provides a flow-independent estimate that is increasingly used to confirm severity and inform timing.
- Fifth, the patient. Age, comorbidities, life expectancy, the presence or absence of a bicuspid valve, the practicalities of life and work, and the patient’s own informed preference about a course of action. Shared decision-making is not a procedural courtesy in Stage C; it is an essential clinical input.
These inputs are weighed together by a Heart Team, an interventional cardiologist, a cardiac surgeon, and a cardiac imaging specialist in a formal review of the case, and the recommendation that follows reflects that collective judgement. Patients are entitled to ask whether their case has been reviewed in this manner, and to expect a clear answer.
A note on the Indian patient
Patients with aortic stenosis in India present, in many cases, considerably younger than the Western registries would suggest. A meaningful proportion of patients reaching valve intervention in this country are in their fifties or early sixties, often as a consequence of a bicuspid valve or the legacy of rheumatic disease. For these patients, the Stage C decision carries an additional dimension, that of lifetime valve management. The valve chosen now, the route by which it is delivered, and the anatomical implications of that choice for any future second procedure all become more consequential when the patient before us has decades, rather than years, of post-intervention life ahead. The framework set out in the global trials remains applicable; the conversation that surrounds it requires particular care in the younger patient.
What I would ask every reader to take from this
To the patient or family: If you have been informed that you have severe aortic stenosis and that your cardiologist has recommended a period of careful surveillance, please understand that surveillance is itself a clinical decision, not the absence of one. Three questions are reasonable to ask, ideally with answers recorded in your medical file. What specifically is being monitored, and on what schedule? What change at the next echocardiogram, or what new clinical finding, would alter the recommendation? And whether your case has been reviewed by a Heart Team, with a clear answer as to who has been involved in that review. If a defined threshold is crossed at the next study, a fresh Heart Team review is the appropriate next step.
To the trainee: Hold on to the distinction between asymptomatic and symptom-concealed. It is the most clinically useful refinement available in this disease. AVATAR, RECOVERY and EARLY TAVR are essential reading in the original. The threshold for intervention in Stage C is moving earlier as you train in the field, and the patient you treat in 2030 will be a different patient from the one your seniors were trained to treat.
To the colleague: I would value the room’s thinking on how strain imaging, biomarker trajectory and valve calcium scoring are being integrated into your own Stage C decision-making, and where the threshold for action is now settling in your practice. The international standard is converging but has not yet converged; the conversation among senior operators is, in my view, the most productive place to keep refining it.
“Severe describes the valve. Symptomatic describes the patient. Stage C is the space between, and it is no longer a space in which clinical surveillance, on its own, is sufficient.”

