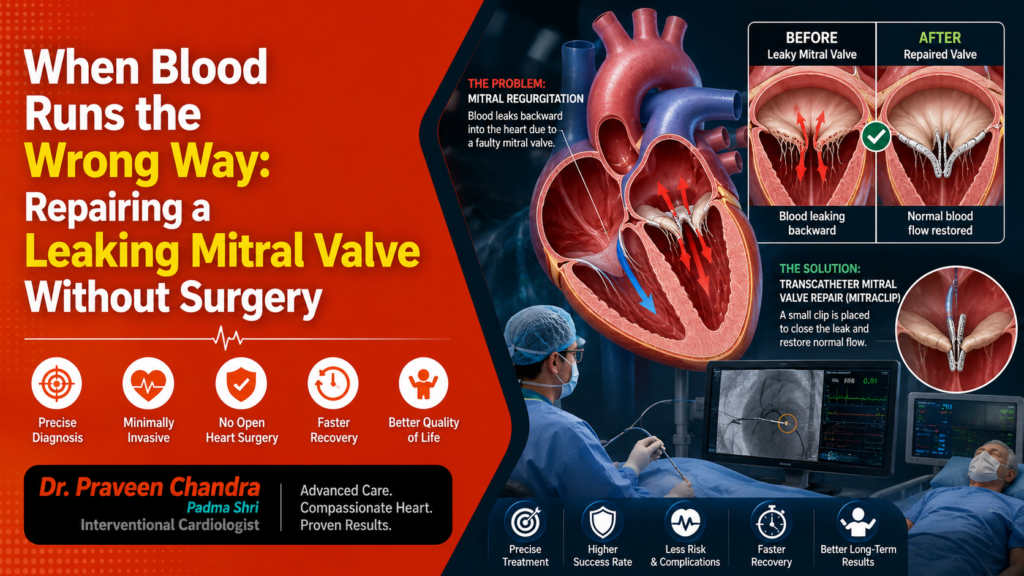
The healthy heart obeys one unbending rule. Blood moves forward and never back. Four valves enforce it, four doors that swing open to let blood pass and fall shut to stop it returning. When I am asked about a leaking mitral valve, I find myself thinking about that rule, and the one quiet place it has broken. The mitral valve guards the entrance to the heart’s main pumping chamber. When it no longer seals, a share of every heartbeat travels back the way it came, toward the lungs, instead of out to the body. We call this mitral regurgitation. Nothing about it hurts, and that is precisely what makes it dangerous.
Why a Backward Leak Is So Easy to Miss
The heart is loyal to a fault. Faced with a leak, it does not protest. It works harder, pumping the wasted blood a second and a third time to cover the shortfall, and for years it succeeds. The price is paid slowly and out of sight. The lungs grow a little congested, so a familiar staircase begins to feel longer. The chambers stretch to hold the extra volume, so the rhythm can tip into atrial fibrillation, that fluttering, irregular beat. Often the very first clue is one the patient never feels, a soft murmur a doctor catches through the stethoscope, which is simply the sound of blood slipping backwards. By the time breathlessness grows hard to ignore, the heart has usually been carrying the leak for a long while. One fact deserves to be fixed in the mind. No tablet can reseal a valve. Medicines can drain the congestion and calm the rhythm, yet a severe leak is a mechanical problem, and a mechanical problem needs a mechanical answer.
Two Ways the Door Fails, and Why the Cause Decides the Cure
A mitral valve leaks for one of two very different reasons, and telling them apart is half the work. In the first, the valve itself has worn out. A leaflet billows back like a slackened sail, or perhaps one of the delicate cords anchoring it snaps, leaving the two halves of the door unable to meet. This is a primary leak, a fault in the valve. In the second, the valve is intact, but the muscle around it has enlarged and weakened, usually after years of high blood pressure or a previous heart attack, until the opening is stretched too wide for the leaflets to close across it. This is a secondary leak, a fault in the heart that the valve only reveals. The distinction is far from academic. It decides whether the real target is the valve, the heart muscle, or a measure of both.
How I Decide: Surgery or the Clip
This is where I have to be exact, because the choice turns on two clear questions rather than on instinct. The first we have already met. Is the leak a worn valve, a primary leak, or a stretched heart, a secondary leak? The second is just as decisive. Can this patient safely undergo open-heart surgery? That second question, surgical risk, is the line that divides most of my patients. A well-made surgical repair outlasts anything I can offer through a catheter, so when someone has a primary leak, a valve that can be repaired, and a body that can withstand the operation, I send them to the surgeon without hesitation. For a younger or otherwise healthy person, that durability is worth far more than the smaller scar of a catheter. The catheter comes into its own only when the surgeon’s route is closed.
Mending a Valve Through a Vein
For those patients, we can now repair the valve without opening the chest at all. The procedure is transcatheter edge-to-edge repair, known to many by its device, the MitraClip. We pass up through a vein in the leg and into the heart, then cross from the right side to the left through the thin wall that divides the upper chambers. From there, every movement is guided by three-dimensional echocardiography, a live ultrasound image of the valve rendered in real depth, because at this scale the eye needs more than a flat picture. We carry a small clip to the leaking edges and draw the two leaflets together at the point where they fail to meet. One wide leak becomes two narrow channels that seal, and on the screen the backward jet shrinks and then vanishes. Sometimes a single clip settles it, and sometimes the valve asks for a second. The patient is lightly sedated, feels almost nothing, and is usually walking the next day.
The Patients the Clip Was Made For
Two groups, in the main. The first is the patient with a primary leak, a genuinely worn valve, whose surgical risk is simply too high because of advanced age, a weakened heart, frail lungs or kidneys, or a chest that has been operated on before. Surgery would endanger them, so the clip offers a repair their body can actually tolerate. The second group, and this is where the strongest evidence sits, is the patient in heart failure whose leak is secondary, driven by a heart that has stretched out of shape. For them, careful trials have shown that closing the leak with a clip, on top of the right medicines, can ease symptoms and lengthen life. In every case the choice is made by a heart team, surgeons and imaging specialists and anaesthetists studying the same scans together, because with a leaking mitral valve the judgement is harder than the procedure.
What the Evidence Actually Says
I am careful with the word safe, so here is the evidence in its place. In patients with heart failure and a secondary leak, a landmark trial called COAPT showed that adding the clip to the best available medicines cut hospital admissions and improved survival, and the 2025 European guidelines now rank it among their firmest recommendations for these patients. For high-risk patients with a worn valve, the clip reliably reduces the leak and gives back breath, with a low risk of serious complications. It does not yet promise the decades of durability that a fine surgical repair can, and that single honest sentence is the reason we choose it for some patients and not for others. Safety, in this work, is mostly a matter of choosing well.
The Breath That Comes Back
The first thing a patient notices is the return of their breath. Within just a few weeks, the staircase that once felt like an insurmountable climb softens into an easy walk. This happens because the heart is finally cured of an exhausting flaw; it has stopped pumping the same blood twice. For those who had been trapped in a cycle of hospital visits with fluid pooling in their lungs, life suddenly opens up as those admissions finally begin to thin out. The path forward is simple, sensible upkeep: staying consistent with the heart medicines that keep the system strong, and checking in once a year with an echocardiogram to ensure the valve and the clip are doing their job perfectly. Precision care doesn’t end when you leave the hospital. For the right person, an afternoon’s work can return a whole season of ordinary, unlaboured living.
Why the Decision Matters as Much as the Device
More than almost anything else I do, a leaking mitral valve rewards judgement. The same clip is a quiet triumph in the right patient and a missed chance at a better operation in the wrong one. That is why experience here matters beyond the steadiness of the hands. I performed India’s first percutaneous mitral valve repair, when the very idea of mending a valve through a vein was still met with doubt, and I have spent the years since helping the field find its feet in this country and teaching those who will carry it forward. At Medanta, the choice is weighed inside a structural heart programme two decades in the making, with a full heart team and the three-dimensional imaging this repair leans on entirely. The device has become dependable. The decision is where the care still lives.
If a doctor has ever mentioned a murmur over your heart, or if stairs that once meant nothing have started to ask something of you, please do not let it fold quietly into the years. Ask for an echocardiogram. It is painless and brief, and it can catch a leak while it is still only a sound, long before the heart has paid for keeping it secret.
Dil Se,
Dr. Praveen Chandra

